Among the mysteries of Alzheimer's disease is the elusiveness of diagnosis. Psychological exams can be given, brain-imaging scans can be used, and laboratory tests can be ordered. A neurologist or other specialist can use these to make a "probable" diagnosis. But for Alzheimer's disease and similar dementias, definitive markers do not exist.
Alzheimer's disease was first identified by German physician Alois Alzheimer in 1906 after the death of a 51-year-old female patient who had suffered from extreme cognitive impairment. An autopsy revealed a brain riddled with amyloid plaques and neurofibrillary tangles, which are still the physiological hallmarks of the disease. Medical knowledge has evolved greatly since then, but these abnormalities cannot be identified in living patients. Diagnosis depends largely on inexact expressions of behavior.
When it comes to aging and brain function, "there are many shades of gray," says Marsel Mesulam, professor of neurology and director of Northwestern's Cognitive Neurology and Alzheimer's Disease Center. Variables are as innumerable as the brain is complex. "This is where clinical judgment comes in."
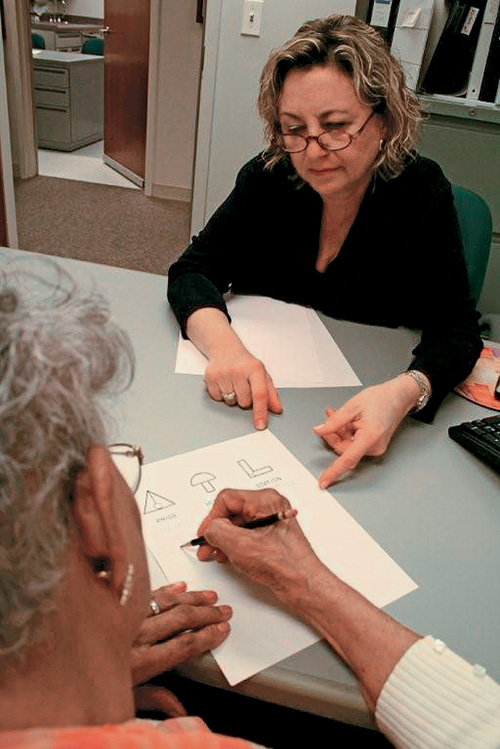
"To distinguish when so-called normal aging ends and when abnormal aging starts," Mesulam says, "there is a collection of tests." Sometimes having patients listen to words and repeat them reveals the dilution of short-term memory. Drawing relatively simple forms with pencil and paper suggests a patient's sense of spatial relationships. Procedures such as MRIs and CT scans provide added indications that figure into a diagnosis. Beyond this, chemical tests and an inventory of medications that the patient is taking can provide clues of non-Alzheimer's causes for Alzheimer's-like symptoms.
A patient's detailed medical history remains key to diagnosis of Alzheimer's disease and comes only from the patient or from people who know him or her. Clinicians will consider education and "previous level of achievement" when examining patients for Alzheimer's.
"If at the age of 75 or 80 you are still running your family company, and you suddenly have a problem understanding payroll, that's a problem," Mesulam says. "On the other hand, if you have a [lesser] set of responsibilities or achievements and at that age can't understand complex numbers, that may mean nothing."
While forgetfulness is the most common mental lapse of most dementias, symptoms vary widely. Other warning signs include poor concentration, trouble finding words and "almost always a detachment from family and usual interests," Mesulam says. Yet he insists that people looking for dramatic indications may be waiting a long time. "By and large, Alzheimer's is a bland disease that makes people less and less competent at what they once did well."
Because of its slow progression, accurate diagnosis of Alzheimer's disease requires the same communication skills that also greatly enhance treatment. While patients are often unhelpful because they are unaware of symptoms or because they react to them with anger, it falls to family members to describe behavioral abnormalities occurring in a patient.
"But sometimes it's the spouse who wants to deny the presence of change," Mesulam notes. So familial and social relationships can facilitate or impede diagnosis, just as those relationships figure into the treatment or management of the disease. Consequently, family dynamics remain just one of the deep complexities of the still-dark medical frontier of Alzheimer's disease and dementia.— J.P. |